
Technologiebasierte Interventionen und Faktoren, die die Einhaltung von subakuten Schlaganfallpatienten im Heimübungsprogramm beeinflussen
Abstract
Background: Cerebrovascular accident is a life-threatening disease, linked with long-term physical and neurological disabilities. Physical activity is an essential action in treating and recovering from long-term disabilities of a stroke event. Home exercise programs (HEP), are a valuable tool for the rehabilitation of sub-acute stroke patients, done at their homes. However, adherence is still a major barrier to the success of HEP. Therefore, comprehending the reasons and factors that affect the compliance of this type of patient in their home setting is a key aspect to increasing their adherence and the potential success of the HEP.
Objective: To determine the most common enablers and barriers to physical activities in home settings, and potential interventions to increase the adherence of patients in those environments.
Methods: Search was performed using CINAHL, Google Scholar, PubMed, PEDro, and Cochrane databases. Relevant articles were screened by title and abstract, followed by full-text screening for inclusion/exclusion criteria and of methodological quality assessment. Data was systematically extracted and synthesized using thematic analysis.
Results: Four randomized controlled trials and five qualitative studies met eligibility criteria. The three most important motivator (enablers) for HEP was ‘knowledge’, ‘health care provider’, and ‘social’. The three most important barriers for HEP were ‘physical capability’, ‘health care provider’, ‘motivation’. Technology-based interventions were effective in improving stroke patients’ adherence, physical capacities, and quality of life.
Conclusion: This review highlighted the importance of implementation of technology-based interventions onto HEP and long-term educational strategies for the stroke patient and close related family and caregivers to increase the adherence and success of HEP.
© Amsterdam University of Applied Sciences, All rights reserved.
Keywords: stroke, Physical Therapy Modalities, Rehabilitation, physical functionality
Introduction
Cerebrovascular accidents are health problems that can be lethal or cause severe physical and neurological disabilities. The level of the impairment or disability is related to the severity of the brain lesion, the time spent to start the treatment during a stroke event, and the early start and effectiveness of the rehabilitation program during the first six months after the event (Gbiri et al. 2014).
Stroke is the second cause of mortality worldwide; 50% of survivors become chronically disabled (Donkor 2018). Moreover, due to the aging population, it is predicted that direct stroke costs will increase by 238% until 2030 in the USA, more than any other important cardiovascular disease such as hypertension, heart failure, or coronary heart disease (Heidenreich et al. 2011). This prediction draws attention to the health care sector in order to reduce and prevent stroke accidents and to introduce more effective and efficient rehabilitation programs.
From a physiotherapeutic perspective, it is important to increase the efficiency of the rehab programs in order to increase the chances of patient recovery in the first 6 months (Cauraugh and Summers 2005; Lee et al. 2015). Likewise, it is important to develop programs that accelerate hospital discharge in the acute phase, aimed at rehabilitating patients to a functional level of independence (Miller 2009). This will make it possible to transfer physiotherapy rehabilitation in the sub-acute or chronic phase to clinics or home settings.
A common approach to rehabilitation in the home setting is via home exercise programs (HEP). HEP is a rehabilitation program performed in the patient’s home, with the assistance of a physiotherapist in person or remote, or with videos or paper-based guides, showing the exercise routine and how to perform them. HEP has shown to be a valuable addition to the conventional center-based program (CBP), which includes rehabilitation programs done in a physiotherapy clinic with the close assistance of one or more professionals. HEPs have several benefits in terms of continuation of the treatment, time and commuting efficiency, cost-efficiency, participation and integration among caregiver, family, and patients, as well as the effectiveness of the long-term rehabilitation results (Oddy and da Silva Ramos, 2013; Novak and Berry, 2014; Paleg and Livingstone, 2015).
HEP has shown numerous benefits for stroke patient recovery. However, adherence is a crucial factor determining the success and the time spent in rehabilitation (Ogwumike et al. 2014). Adherence or compliance is defined as “the extent to which a person’s behavior – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider” (Sebate 2001). In other words, it is the voluntary participation of a patient with behavior actions that promote a preventive and a positive therapeutic outcome. From a physiotherapy perspective, compliance of patients embraces their attendance to appointments, the performance of the given exercise programs or other interventions, frequency, execution, pace, range of motion, and other specific prescribed parameters (Jack et al. 2010).
Based on previous evidence, we know there is a close relationship between the level of adherence of patients and their recovery outcomes at the end of the treatment (Imayama et al. 2013; Gunnes et al. 2019). The more compliant and consistent with the program, the better the results. In chronic conditions prescribed HEP often meets low adherence, which negatively impacts the success of the program (Bassett. 2003). Other impacts of poor compliance are potential reduction of the effectiveness of the CBP, increased progression of the disease, reduced quality of life or even recurrence of stroke, and higher death rates (Peschin. 2010).
Since patient’ adherence is one of the major factors that affect the successful implementation of HEP’s, and there is only limited research targeting specifically subacute stroke patients, we believe understanding the factors affecting the compliance of this type of patient in their home setting is a key aspect to increase their adherence.
Therefore, it is crucial to investigate the factors influencing the level of adherence, such as practice recommendations, frequency, intensity, type and complexity of exercises, motivation, the level of patient limitation, socio-economic or other factors that might facilitate or hinder sub-acute stroke patients in performing HEP. This review is likely to help physiotherapists to reduce time and costs spent on rehabilitation and ultimately improve the quality of life, functionality, and independence of patients. Therefore, its aim is to answer the following research question: How can adherence be optimized in a home-exercise program for physiotherapeutic rehabilitation of subacute stroke patients?
Methods
Data sources and the search string
A systematic literature search was conducted in the following five databases: Pubmed, Cochrane, PEDro, CINAHL, and Google Scholar. The electronic search was conducted over a two months period, starting April 12, 2021. Randomized controlled trials (RCT’s) and qualitative studies were included in this review. The relevant keywords used for this review were chosen using the PICO (population, intervention, control group and outcome) framework for RCTs (Considine et al. 2017) and the SPIDER (sample, phenomenon of interest, design, evaluation, research type) framework for qualitative studies (Cooke et al. 2012). An overview of all search results and combinations of keywords as well as individual search strings can be found in Appendix B.
The following keywords were used: “Adherence”, “stroke”, “home” “exercise”.
The following synonyms for the keywords were used:
Keyword 1: Adherence OR compliance
Keyword 2: Stroke OR CVA OR Cerebrovascular Accident*
Keyword 3: Sub-acute OR subacute OR chronic OR late rehab*
Keyword 4: Home OR home-setting OR home setup
Keyword 5: Exercise OR exercise program OR rehab* OR Physiother*
Keywords and synonyms were used in connection with Boolean operators “AND”, “OR” and trucking (*). The final keywords per database are as follows:
Pubmed
Adherence OR compliance AND Stroke OR CVA OR Cerebrovascular Accident* AND Sub-acute OR subacute OR chronic OR late rehab* AND home OR home-based OR home setup AND exercise OR exercise program OR rehab* OR Physiother*
Results: 25
Filters: 10 years, English, RCT
PEDro
Exercise rehab* stroke home adherence
Results: 4
Filter used: neurology in the sub-discipline, 5 years, English, RCT
Cochrane
Rehab* AND stroke AND home AND adherence AND exercise program
Result: 48
Filter: 10 years, English, RCT
Google Scholar
Exercise stroke adherence home
Filters used: 10 years, all in title
Results: 10
CINAHL
Exercise, stroke, adherence, home
Filter: 10 years
Results: 4
Search strategy and study selection
The final articles were selected by the main reviewer (CW). The selection process started matching the keywords and their synonyms with the Boolean operators AND, OR and trunking (*) for each search database. Then, additional filters were applied: English, 2010 and above, RCT. The articles were then screened by title and abstract, after which duplicates were removed. The references of included studies were scanned to identify and ensure other relevant studies were selected. The remaining articles were then checked on inclusion and exclusion criteria, and, lastly, assessed for quality to complete the selection procedure.
Inclusion & Exclusion Criteria
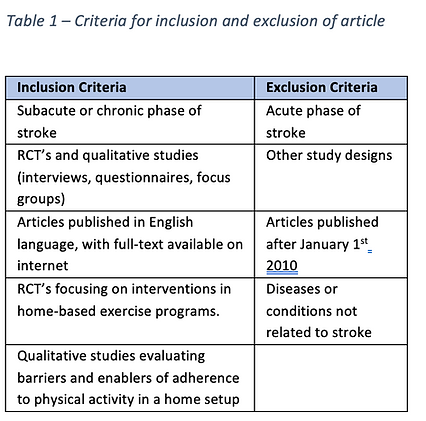
In order to narrow the research and find articles that could answer the research question, inclusion/exclusion criteria were developed and applied during the study selection. Articles were included only if full-text was available and written in the English language. Primarily, the search strategy was made to include only RCTs. However, due to few RCT studies available, qualitative studies were also included. This inclusion was also based on the relevancy of the qualitative studies found, which were in line with the idea of this review and potentially supportive of the answer to our research question.
In order to include articles with recent and relevant information, with potential practical application, only studies published after January 1st, 2010 were selected. The target population for all studies should have suffered minimally one stroke and be on the sub-acute of a home-based rehabilitation program. For RCT studies, the therapy intervention should be focused on an exercise program. For the qualitative studies, the phenomenon of interest should be focused on barriers or enablers of adherence in HEP. Table 1 (below) shows a complete list of inclusion/exclusion criteria.
Data extraction
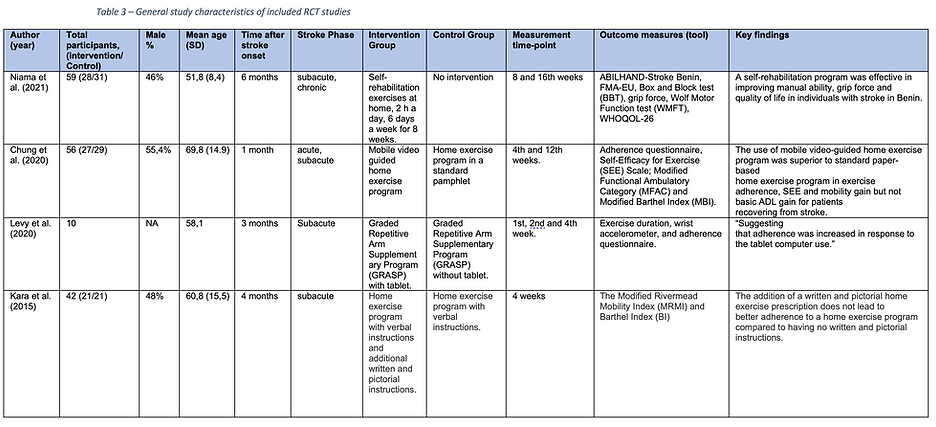
Data extraction was carried out by the main reviewer (CW). For the RCTs, data extraction contemplated Population (age and gender percentage), Characteristics of stroke (time after stroke onset and stroke phase), Interventions (exercise program, control group, measurement time-point, and measurement tools), and Key findings (Table 2).
In order to extract meaningful data from the qualitative studies, the JBI qualitative data extraction tool (Joanna Briggs institute 2019) was used as a guiding reference (Table 3). Data extracted included Population (age and gender percentage), Stroke phase, Data collection method, Phenomenon of interest, and Key findings. Data synthesis was extracted by analyzing the study outcomes and interpreting direct quotations of patients. Relevant results, words, sentences, patient’s opinions, and beliefs related to the phenomena of interest were gathered and grouped into categories (themes) to facilitate final data interpretation and conclusion.
Quality assessment
Quality appraisal of individual studies was done using the PEDro scale for RCTs, based on its reliability in the field of physiotherapy, and as a practical tool to assess randomized controlled trials (Maher et al. 2003). The PEDro scale is a quality appraisal tool, composed of 11 items, with each item worth one point. Studies considered of “good” quality need to score 6 or above (Peng et al. 2019). In this review, only articles with a score of 6 or higher were included.
Appraisal of qualitative studies was done via the Critical Appraisal Skills Programme (CASP) tool (CASP 2018). This tool was chosen because it is a common quality checklist for qualitative studies (Long et al. 2020). The CASP is composed of 10 questions, and each question can be answered “yes”, “no” or “can’t tell”, and a comment section is provided. This tool does not recommend a final cutoff score to ensure the quality. However, it was determined that each article should have at least six answers “yes” to be considered in this review. To avoid evaluation bias, two graders (CW and AB) independently applied the tool, then compared results, discussed contradictory answers, and decided on the final grading together.
Results:
Study selection
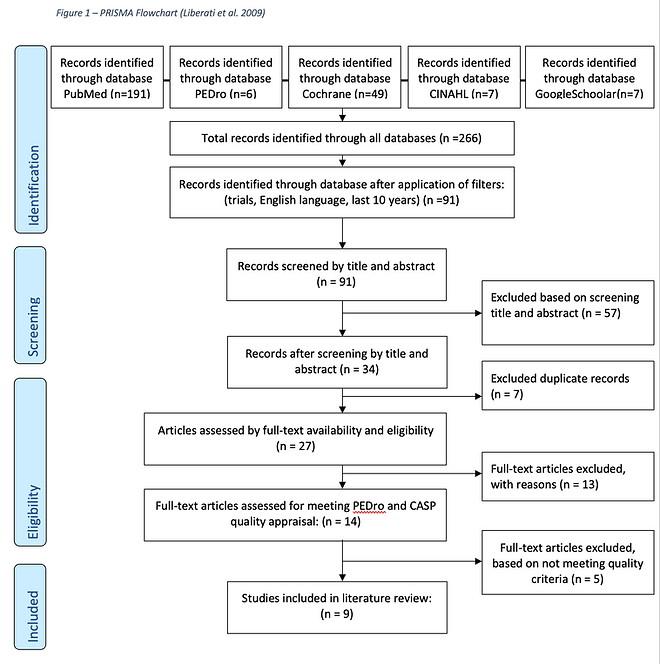
Initial search results in all databases (Pubmed, Cochrane, PEDro, CINAHL, and Google Scholar) yielded 266 studies, using the final keyword terms. After additional filters were applied, 91 studies were identified for the screening process and duplicate check. Of these, 27 were applicable for full-text review. Only 14 studies fulfilled the eligibility criteria and 9 articles were finally selected after performing the quality check: 4 RCTs and 5 qualitative studies. Figure 1 outlines the process of selection and exclusion of articles through the PRISMA flowchart (Liberati et al. 2009).
Methodological quality
The methodological quality for the RCTs was assessed using the PEDro scale (Maher et al. 2003). Studies were considered acceptable if they reached 6 points or above Peng et al. (2019). Table 2 depicts the final grading for RCTs. PEDro key criteria for quality assessment are described in appendix A. The methodological quality of the qualitative articles was checked by the main researcher (CW) in consultation with an external reviewer (AB). They applied the CASP tool for Quality Assessment (CASP 2018). All studies met satisfactory quality, being answered “no” or “can’t tell”. See Table 3 for grading results. CASP key criteria for quality assessment is described in appendix A.
Participants
Studies included a total of 503 participants, with a mean age of 60,19 years old. The average male % was 56,1, and the age ranged from 16 to 80 years old.
Focusing only at the RCT studies, they presented a total of 167 stroke survivor patients. The average age range between the studies was 60 years old. The average male percentage ranged from 46 to 55%. Time after the onset of stroke ranged between one to six months. All patients were in the sub-acute phase.
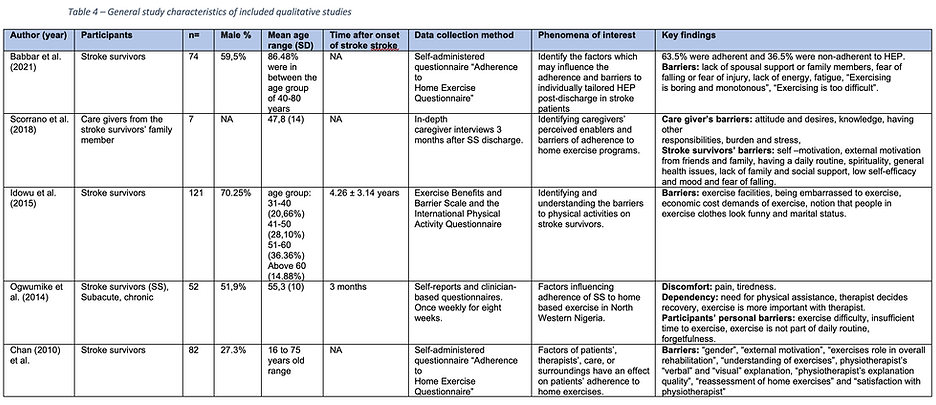
Focusing only at the qualitative studies a total of 336 stroke survivor patients were presented. The percentage of male were around 50%. The age ranged between 16 years (Chan et al. 2010) to 80 years old (Babbar et al. 2021), with the majority of patients falling under 40 to 80 years old. One study (Scorrano et al. 2018), provided the perception of caregivers (n=7) towards the stroke patients they were taking care. The others focused on the actual stroke patients.
Study characteristics
A description of the characteristics of included studies can be found in Tables 3 (RCTs) and 4 (qualitative studies). Apart from general characteristics, the studies will be described separately for a better representation of findings.
Time
The timeline for individual studies ranged from the first to the 16th week post onset. Data collection point varied from 3 months (Ogwumike et al. 2014) to 4 years (Idowu et al. 2015) after stroke. The data collection method was done by Self-reports and clinician-based questionnaires. The questionnaires were based on validated tools (Bassett, 2012 & 2003) and modified versions. The phenomena of interest focused on barriers, enablers, self-efficacy and intention of exercise in home setup.
The phases of stroke are generally classified as the time after the stroke event. The phases are divided in: acute (first two weeks); subacute (from 3-11 weeks), when the most of changes and improvements occur; early chronic phase (from 12-24 weeks) and lastly the chronic phase (from 24 weeks after onset) (Bonita & Beaglehole, 1988; Horstman et al. 2012; Cramer, 2008; Rehme et al. 2012).
Outcome measures
A great variety of measures tools were used. The exercises volume was measured by smartwatches, counted in met minutes (Levy et al. 2020). Patient’s mobility was measured with The Modified Rivermead Mobility Index (MRMI) and Modified Functional Ambulatory Category (MFAC) (Kara et al. 2015; Chung et al. 2020). Dexterity and activities of daily living was measured with Box and Block test (BBT), grip force, Wolf Motor Function test (WMFT) and Barthel Index (BI) and a modified version (MBI) (Kara et al. 2015; Chung et al. 2020); Niama et al. 2021). To measure adherence, logbooks, wrist accelerometer, self-reported questionnaire were used.
RCT studies
The RCT studies were divided, for better comprehension, into technology-based interventions and the studies who did not use technology as part of the interventions.
Interventions with electronical device:
-
Mobile video guided home exercise program Chung (2020). Control group received home exercise program in a standard pamphlet.
-
Graded Repetitive Arm Supplementary Program (GRASP) with tablet Levy (2020). Control group received graded Repetitive Arm Supplementary Program (GRASP) without tablet.
Intervention without electronical device:
-
Self-rehabilitation exercises at home with equipment kit, which included the material required for performing the exercises, a daily notebook, and the self-rehabilitation protocol, with pictures describing all exercises Niama (2021). Control group received home exercise program only with verbal instructions.
-
Home exercise program with verbal instructions and additional written and pictorial instructions Kara (2015). Control group received home exercise program only with verbal instructions
Key findings
The key findings were divided into RCT and qualitative to ease the comprehension of the reader.
RCT key findings
A self-rehabilitation program was effective in improving manual ability, grip force and quality of life in individuals with stroke (Niama et al. 2021).
The addition of a written and pictorial home exercise prescription does not lead to better adherence to a home exercise program compared to having no written and pictorial instructions. (Kara et al. 2015).
The use of mobile video-guided home exercise program was superior to standard paper-based home exercise program in exercise adherence, SEE and mobility gain but not basic ADL gain for patients recovering from stroke Chung et al. (2020).
The use of visual feedback, via a tablet computer, increased the time stroke patients spent doing physical activity, which may indicate an increased adherence to the exercise program (Levy et al. 2020).
Qualitative key findings
The data synthesis generated 10 themes, which represented the key findings related to the success (enablers) or failure (barriers) to adhere to HEP. Based on the total number of direct quotations found, the three most important motivator (enabler) for HEP was the (1) ‘knowledge’, (2) ‘health care provider’, and (3) ‘social’. The three most important barriers for adhering to HEP were (4) ‘physical capability’, (5) ‘motivation’ and ‘health care provider’. Only the five most important factors were described below, see table 5, for the complete list obstacles and facilitator and how they were defined.
-
‘Knowledge’: Embraces the technical information from patient and health care provider on physical activity and how the patient understands the benefits from exercising for a post-stroke condition.
-
‘Health care provider’: the informal (family member) and/or health professional technical quality and attitude towards the patient.
-
‘Social’: The active or passive help, involvement and integration between family and friends towards the patient.
-
‘Physical capability’: The physical functionality, fitness, motoric and cognitive factors that influence physical activity of patients.
-
‘Motivation’: Embraces patients’ self-efficacy, emotions, moods and intention/willingness towards physical activity and the overall post-stroke condition.
Discussion
The analysis of our results shows the relevancy of adding technology-based interventions in order to increase adherence in sub-acute stroke patients. The other important finding of this review stated the most common adherence barriers or enablers to HEP. Our aim in this review, was to optimize adherence of sub-acute stroke patients on home-based exercise programs.
The present study found that besides the increase on adherence, manual ability, grip force, mobility, time spent doing physical activities, self-efficacy and quality of life of stroke patients was enhanced. That is aligned with prior researches (Simpson et al. 2019; Imran et al. 2021) that found similar results when technology-based interventions were applied on stroke and other cardiovascular patients, in home-based rehabilitation program, increasing adherence, as well as physical, motor and quality of life aspects (Linder et al. 2015; Coulibaly et al. 2018).
The success of technology-based HEP can be explained due to its versatility, reach extension and lower costs when compared to conventional face-to-face treatments. Remote technology is used to provide more information and knowledge. Electronic schedules and automated messages, help patients to remind their medications increasing their compliance (Vervloet et al. 2012), and could potentially do the same on increasing exercise adherence (Crayton et al. 2018). Another relevant aspect of implementing technology on rehabilitation programs, is to be better cost-effective on treatments. Transporting patients and health care providers represents a great part of health expenses in rehabilitation programs, Telerehabilitation is an alternative, which reduce drastically the time and commuting costs, especially in continental sized countries or isolated and remote areas, connecting health professionals to patients instantly (Thaker et al. 2013; Lloréns et al. 2015). In addition, this allows patients to have access to more information, knowledge and treatments that they wouldn’t have access if it wasn’t for the ease of technology (Yan et al. 2021).
The mean age of the population of our review was above 60 years old. That corroborates with (Kelly-Hayes 2010), which says 75% of stroke occurs in people above 65 years old. That arise an important aspect needs to be taken in consideration when implementing a technology-based rehabilitation on elder patients. These populations are more prone to present physical and cognitive impairments, affecting the usage of technology during HEP (Smith A, 2014) and older adults are slower to adopt newer technologies than younger adults (Czaja et al. 2006).
However, in contrast, this study (Ciccone et al. 2021) found a great engagement and utilization of technology devices such as computers, tablets, smartwatches, and smartphones by elder stroke population. Besides, the currently young population, which have more affinity and uses technology more frequently, will eventually get older and be more likely to use technology devices for health and rehabilitation purposes.
The present study also focused in finding the main barriers and enablers to adherence of HEP by stroke patients. This information is crucial to understand, develop and act on changes on patients’ lives, targeting the obstacles and promoting the facilitators. This is aligned with several studies, focused on stroke, or other chronic conditions (Nair et al. 2011; Okwose et al. 2020; Torriani-Pasin et al. 2021).
The most important barrier found was the theme ‘physical capability’ of patients, comprehending motor impairments, fatigue, pain, stiffness, swelling, nausea, weakness among others. This finding is also reported by (Duncan et al. 2012; Ogwumike et. al 2014; Ogwumike et. al 2015). This barrier, according to Loureiro et al. 2014, is determinant in progressively disabling patterns and consequently reduction of physical activity and fitness. Therefore, targeting actions to improve ‘physical capabilities’ barriers can be determinant to the success of the rehabilitation, decreasing death rates and preventing stroke reoccurrences (Wendel-Vos et al. 2004). An effective method to improve ‘physical capabilities’ is to develop exercise programs tailored specifically to the patients’ need, taking in consideration their economic and environment circumstances, personal situations and preferences (Collado-Mateo et al. 2021).
An important finding of this review, is that ‘health care provider’ can work as a barrier and/or an enabler to patient adherence. Informal carers, are often close family members who take the responsibility to care for the stroke patient. Usually, due to accumulation of duties, lack of knowledge, work, stress and social pressure to care, impacts patients’ adherence negatively. However, on the other side, the willingness to assist, the close relationship bond and the desire for the family member to improve were factors affecting adherence positively. The study from Martin et al. 2005, also found that the relationship care provider – patient, is crucial, since promotes patient fulfillment and approval, leading to lower nonadherent outcomes and improvement in overall health status. This theme is also liked closely to another theme, ‘social’.
Another theme that had positive and negative impacts was ‘motivation’ of patient. Improvement was noticed when patient had the willingness or was encourage to return to walk, perform activities of daily living, to work and other activities executed as independently as possible, as it was done before the stroke. This is in accordance to Rodrigues et al. 2018, which states that higher senses of motivation and accomplishments, promote a higher adherence, which improves the patient’s quality of life, and as a positive cycle, giving them more motivation to continue. On the other hand, feelings of frustration, low self-efficacy, fear, embarrassment to exercise and having too low or too high expectations, were obstacles hindering patient’s adherence to exercise (Eynon et al. 2019; Collado-Mateo 2021). According to Tierney et al. 2011 and Alvarado et al. 2015, especially in chronic diseases and on health conditions where there is a loss of control of your physical and/or cognitive capabilities, such as multiple sclerosis and stroke survivors, adherence is decreased due to depressive and helplessness emotions, and to not feel capable of promote changes on your own life (Abramson et al. 1978; Thompson et al. 2016; Vseteckova et al. 2018).
Another important result of this review, found the theme ‘Knowledge’ of patient and health care provider as the major enabler to improve adherence. Factors such as patient comprehension of the role of exercise and the importance of physical activity on the success of the rehabilitation is also found correspondingly in literature (Jasmine et al. 2012; Ghisi et al. 2020); and the knowledge of health professionals on what, when and how to prescribe exercises and effectively transmit it to the patients, were major factors influencing adherence, and can be found similarly in previous publications (Simek et al. 2012; Jansons et al. 2017; Shore et al. 2019).
Lastly, it is important to take in consideration the power and effectiveness education have on the success of every rehabilitation program for stroke survivors or other type of patients. Education as an intervention have shown increased self-efficacy, adherence, and consequently physical, emotional and improvement in the overall health of patients (DeWalt et al. 2004; Bhat et al. 2010; Harrington et al. 2010) Therefore, it is crucial and clinically relevant to identify the barriers and enablers, as this research did, but also to promote the education based on the identified factors to increase the success of the rehabilitation.
Limitations
The main limitation of this study was the difficulty to find recent literature focused specifically on sub-acute stroke patients’ adherence to HEP. Since it is a very specific population and intervention, only a few RCTs were found, therefore, qualitative studies were decided to be included. The decision of including qualitative studies, could have brought a different search string, and possibly a greater variety of studies. That could have helped on the next limitation, which was the heterogeneity of articles found. The final included articles have different baseline features such as age range, time after stroke, physical capacity. Another problem was the different factors and measurement tools used and analyzed by each study, making it difficult to compare between each study. Another important limitation was the different ethnicities, socio-economic status and country (developed and developing) where the studies were conducted, making it difficult to extrapolate one’s results to another region or country. In addition, there was no standard questionnaire for the qualitative studies, also preventing some comparisons between studies. Lastly, adherence, is known to be difficult to measure due to several factors. The limitations of using technology associated with the measurement of adherence, is that there is confounding factor if the adherence to the intervention increased or the adherence or usage of the technology increased, specially when are computer, mobile or tablet related (Sieverink et al. 2017).
Future research
It is recommended to homogenize the population better, including specific age range, type of stroke, equal gender distribution, the stage of rehabilitation and same patient base line. The independent variable, so factors that influence the adherence, must compare same interventions: tools, transmission of information to patient, same training program and parameters, the same retests and follow-up dates. A control group, where no intervention is applied must also be avoided in order have meaningful comparisons. The measurement tool for adherence must also be homogenized, measuring not just the days the patient was active, but also quantifying the volume, time spent and intensity, during the training days.
Conclusion
The use of exercise programs is effective for home-based rehabilitation of stroke patients, leading to physical, functional and quality of life improvements. The implementation of technology interventions via mobile video-guided exercise and via visual feedback on tablet computers, showed higher adherence and increased time spent doing physical activity. The main barriers for adhering to HEP were related to the themes ‘physical capability’ and ‘motivation’ of patients, and the informal ‘health care provider’ burden and stress. The most common enablers were related to the themes ‘knowledge’ on what must be done and what is the importance of exercise, the overall quality of ‘health care provider’ carrying for patients, and ‘social’ support from close family and friends. In conclusion, this study shed a light on which factors do HEP must focus more in order to improve the adherence of their patients and potentially increase cost efficiency, reduce time spent for rehabilitation and ultimately improve the quality of life, functionality and independence of patients by the end of the HEP.
Acknowledgments
The author would like to thank his coach Miriam Wijbenga, PhD candidate and senior lecturer at European School of Physiotherapy, for her guidance and generous feedback. A thanks goes to Esther Verloop, librarian at Amsterdam University of Applied Sciences, who provided the author with guidance. Also, thanks to Katja Fischer, senior physiotherapist at “Gesundheitszentrum Team Physiologic”, for offering us the opportunity to develop our professional product for her practice. Finally, special thanks to Anri Baazovi for being a second reviewer and for all the help and feedback.



Verweise
Abramson LY, Seligman ME, Teasdale JD. Erlernte Hilflosigkeit beim Menschen: Kritik und Umformulierung. J Abnorm Psychol.
1978;87(1):49-74.
Alvarado M, Murphy MM, Guell C. Barrieren und Förderer körperlicher Aktivität bei übergewichtigen und fettleibigen Frauen in einem
Afrokaribische Bevölkerung: Eine qualitative Studie. Int J Behav Nutr Phys Act. 2015;12:97.
Appleby E, Gill ST, Hayes LK, Walker TL, Walsh M, Kumar S. Wirksamkeit der Telerehabilitation bei der Behandlung von Erwachsenen mit
Schlaganfall: Eine systematische Überprüfung. Plus eins. 2019;14(11).
Bassett S. Messung der Patiententreue zur Physiotherapie. Zeitschrift für neuartige Physiotherapien. 2012;02(07).
Bassett SF, die Beurteilung der Patientenadhärenz zur Physiotherapie-Rehabilitation, NZ J Physiother. 2003;31:60.
Bhat A, DeWalt D, Zimmer C, Fried B, Callahan L. Die Rolle von Hilflosigkeit, Ergebniserwartung für Bewegung und Alphabetisierung bei der Vorhersage
Behinderung und Symptome bei älteren Erwachsenen mit Arthritis. Patientenaufklärung. 2010;81(1):73-78.
Bonita R, Beaglehole R. Wiederherstellung der motorischen Funktion nach einem Schlaganfall. Schlaganfall. 1988;19(12):1497-1500.
Cauaugh J, Summers J. Neurale Plastizität und bilaterale Bewegungen: Ein Rehabilitationsansatz für chronischen Schlaganfall. Fortschritte in
Neurobiologie. 2005;75(5):309-320.
Collado-Mateo D, Lavín-Pérez AM, Peñacoba C, et al. Schlüsselfaktoren im Zusammenhang mit der Einhaltung körperlicher Betätigung bei Patienten mit
Chronische Krankheiten und ältere Erwachsene: Ein Umbrella Review. Int J Environ Res Public Health. 2021;18(4):2023.
Considine J, Shaban R, Fry M, Curtis K. Evidenzbasierte Notfallpflege: Entwerfen einer Forschungsfrage und Durchsuchen der
Literatur. Internationale Notfallpflege. 2017;32:78-82.
Cooke A, Smith D, Stand A. Jenseits von PICO. Qualitative Gesundheitsforschung 2012 Oct;22(10):1435-1443.
Coulibaly L., Rochefort C., Kairy D. & Tousignant M. Kosten-Nutzen-Analyse der Telerehabilitation für Menschen, die a
Schlaganfall mit Rückkehr nach Hause ohne intensive Rehabilitation: Eine systematische Überprüfung. International Journal of Hospital-Based Health Technology Assessment. 2018;1:19-44.
Cramer S. Reparatur des menschlichen Gehirns nach einem Schlaganfall: I. Mechanismen der spontanen Genesung. Annalen der Neurologie. 2008;63(3):272-287.
Crayton E, Wright AJ, Ashworth M. Verbesserung der Medikamentenadhärenz bei Schlaganfall-Überlebenden: der Interventionsentwicklungsprozess. BMC
Gesundheitsdienst Res. 2018;18(1):772.
Programm für kritische Bewertungsfähigkeiten. Qualitative CASP-Checkliste; Oxford: CASP; c 2018 [Internet]. Casp-uk.net. 2021 [zitiert am 21. Oktober
2021]. Verfügbar unter: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf
Czaja SJ, Charness N., Fisk AD, et al. Faktoren, die den Einsatz von Technologie vorhersagen: Ergebnisse des Zentrums für Forschung und Bildung
über Alterung und technologische Verbesserung (CREATE). Psychisches Altern. 2006;21(2):333-352.
DeWalt D, Berkman N, Sheridan S, Lohr K, Pignone M. Alphabetisierung und Gesundheitsergebnisse. Zeitschrift für Allgemeine Innere Medizin.
2004;19(12):1228-1239.
Donkor E. Schlaganfall im 21. Jahrhundert: Eine Momentaufnahme der Belastung, Epidemiologie und Lebensqualität. Schlaganfallforschung und -behandlung.
2018;1-10.
Duncan F, Kutlubaev MA, Dennis MS, Greig C, Mead GE. Müdigkeit nach Schlaganfall: eine systematische Überprüfung von Verbänden mit Beeinträchtigungen
körperliche Fitness. Int J Schlaganfall. 2012;7(2):157-162.
Eynon M, Foad J, Downey J, Bowmer Y, Mills H. Bewertung der psychosozialen Faktoren, die mit der Einhaltung der Übungsempfehlung verbunden sind
Schemata: Eine systematische Überprüfung. Skandinavisches Journal für Medizin und Wissenschaft im Sport. 2019;29(5):638-650.
Gbiri C, Akinpleu A, Ogunniyi A, Akinwuntan A, Van Staden C. Klinische Prädiktoren der funktionellen Erholung sechs Monate nach dem Schlaganfall. asiatisch
Zeitschrift für medizinische Wissenschaften. 2014;6(1):49-54.
Ghisi GLM, Rouleau F., Ross MK, et al. Wirksamkeit einer Aufklärungsintervention bei kardiologischen Rehabilitationspatienten in Kanada: A
Multi-Site-Studie. CJC geöffnet. 2020;2(4):214-221.
Harrington R., Taylor G., Hollinghurst S., Reed M., Kay H., Wood VA. Ein gemeindebasiertes Übungs- und Aufklärungsprogramm für Schlaganfälle
Überlebende: eine randomisierte kontrollierte Studie und wirtschaftliche Bewertung. Klinik Rehabil. 2010;24(1):3-15.
Heidenreich P, Trogdon J, Khavjou O, Butler J, Dracup K, Ezekowitz M et al. Prognose der Zukunft von Herz-Kreislauf-Erkrankungen in der
Vereinigte Staaten. Verkehr. 2011;123(8):933-944.
Horstman A, De A, Konijnenbelt M, Janssen T, Gerrits K. Funktionelle Erholung und Muskeleigenschaften nach einem Schlaganfall: eine Vorstudie
Längsschnittstudie. Rehabilitationsmedizin. 2012.
Imran TF, Wang N., Zombeck S., Balady GJ. Mobile Technologie verbessert die Adhärenz bei der kardiologischen Rehabilitation:
Eine Propensity-Score-Matched-Studie. J Am Heart Assoc. 2021;10(15).
Jack K, McLean S, Moffett J, Gardiner E. Hindernisse für die Therapietreue in Physiotherapie-Ambulanzen: Eine systematische Überprüfung.
Manuelle Therapie. 2010;15(3):220-228.
Jansons P, Haines T, O'Brien L. Interventionen zur Erzielung einer dauerhaften Übungsadhärenz für Erwachsene mit chronischen Gesundheitsproblemen, die
ein beaufsichtigtes Übungsprogramm absolviert haben: systematische Überprüfung und Metaanalyse. Klinik Rehabil. 2017;31(4):465-477.
Jasmine TJ, Wai-Chi SC, Hegney DG. Der Einfluss von Wissen und Überzeugungen auf die Einhaltung von Herzrehabilitationsprogrammen in
Patienten mit Herzinsuffizienz: Eine systematische Überprüfung. JBI Libr Syst Rev. 2012;10(7):399-470.
Kelly-Hayes M. Einfluss von Alter und Gesundheitsverhalten auf das Schlaganfallrisiko: Lehren aus Längsschnittstudien. J Am Geriatr Soc. 2010;58
Beilage 2 (Beilage 2): S325-S328.
Lee K., Lim S., Kim K., Kim K., Kim Y., Chang W. et al. Sechsmonatige funktionelle Erholung von Schlaganfallpatienten. Internationale Zeitschrift für
Rehabilitationsforschung. 2015;38(2):173-180.
Levy T, Laver K, Killington M, Lannin N, Crotty M. Eine systematische Überprüfung der Maßnahmen zur Einhaltung körperlicher Vorschriften
Übung Empfehlungen bei Menschen mit Schlaganfall. Klinische Rehabilitation. 2018;33(3):535-545.
Liberati A., Altman D., Tetzlaff J., Mulrow C., Gøtzsche P., Ioannidis J. et al. Die PRISMA-Erklärung zur Berichterstattung über systematische Überprüfungen und
Meta-Analysen von Studien, die Interventionen im Gesundheitswesen bewerten: Erklärung und Ausarbeitung. PLoS-Medizin. 2009;6(7):e1000100.
Linder SM, Rosenfeldt AB, Bay RC, Sahu K, Wolf SL, Alberts JL. Verbesserung der Lebensqualität und Depression nach Schlaganfall
Telerehabilitation. Bin J Occup Ther. 2015;69(2):1-10.
Lloréns R, Noé E, Colomer C, Alcañiz M. Effektivität, Benutzerfreundlichkeit und Kosten-Nutzen eines Virtual-Reality-basierten Telerehabilitationsprogramms
zur Wiederherstellung des Gleichgewichts nach einem Schlaganfall: eine randomisierte kontrollierte Studie. Arch Phys Med Rehabil. 2015;96(3):418-425.e2.
Long H, French D, Brooks J. Optimizing the value of the Critical Appraisal Skills Program (CASP) tool for quality appraisal in
qualitative Evidenzsynthese. Forschungsmethoden in Medizin & Gesundheitswissenschaften. 2020;1(1):31-42.
Loureiro A, Guarita-Souza L, Lerdal A, Langhammer B. Eine Überprüfung der Beziehung zwischen Ermüdung nach Schlaganfall und körperlicher Belastung
Aktivität. Themen in der geriatrischen Rehabilitation. 2014;30(4):296-306.
Maher C, Sherrington C, Herbert R, Moseley A, Elkins M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled
Versuche. Physiotherapie. 2003;83(8):713-721.
Martin LR, Williams SL, Haskard KB, Dimatteo MR. Die Herausforderung der Patientenadhärenz. Ther Clin Risk Manag. 2005;1(3):189-199.
Miller K. Einhaltung des Physiotherapie-Heimübungsprogramms 1-6 Monate nach der Entlassung aus der Physiotherapie durch die Person
Nach dem Schlaganfall. [Master in Wissenschaften]. Fakultät der Indiana University; 2009.
Nair KV, Belletti DA, Doyle JJ, et al. Verständnis der Barrieren für die Einhaltung von Medikamenten in der hypertensiven Bevölkerung durch Bewertung
Antworten auf eine telefonische Umfrage. Patient bevorzugt Adhärenz. 2011;5:195-206.
Novak I, Berry J. Evidenz zur Wirksamkeit von Interventionen im Home-Programm. Physio- und Ergotherapie in der Pädiatrie.
2014;34(4):384-389.
Oddy, M. und da Silva Ramos, S. Kostengünstige Möglichkeiten zur Erleichterung der häuslichen Rehabilitation und Unterstützung. Neurorehabilitation.
2013;32(4):781-790.
Ogwumike O, Badaru U, Adeniyi A. Hindernisse für die Therapietreue bei Schlaganfall-Überlebenden, die ambulante Physiotherapie-Kliniken besuchen
im Nordwesten Nigerias. Klinische Gesundheitsförderung - Forschung und Best Practice. 2015;5(3):4-10.
Ogwumike, O., Badaru, U. und Adeniyi, A. Faktoren, die die Einhaltung von Heimübungen durch Schlaganfallüberlebende im Nordwesten beeinflussen
Nigeria. Internationale Zeitschrift für Therapien und Rehabilitationsforschung. 2014;3(1):8.
Okwose NC, O'Brien N., Charman S., et al. Überwindung von Hindernissen für das Engagement und die Einhaltung einer körperlichen Aktivität zu Hause
Intervention für Patienten mit Herzinsuffizienz: eine qualitative Fokusgruppenstudie. BMJ geöffnet. 2020;10(9):e036382.
Paleg, G. und Livingstone, R. Systematische Überprüfung und klinische Empfehlungen zur Dosierung von unterstütztem Stehen zu Hause
Programme für Erwachsene mit Schlaganfall, Rückenmarksverletzung und anderen neurologischen Erkrankungen. BMC Muskel-Skelett-Erkrankungen. 2015;16(1).
Peng T, Zhu J, Chen C, Tai R, Lee C, Hsieh Y. Aktionsbeobachtungstherapie zur Verbesserung der Armfunktion, Gehfähigkeit und täglichen Aktivität
Leistung nach Schlaganfall: eine systematische Überprüfung und Meta-Analyse. Klinische Rehabilitation. 2019;33(8):1277-1285.
Peschin S., Doane C., Roberts M., Farley M., Gucciardo A., Haddow M., Mintz S., Modica P. Patientenadhärenz: Barrieren erkennen
und Lösungen definieren. Vorteile des American Journal of Pharmacy. 2010;2(2).
Rehme A, Eickhoff S, Rottschy C, Fink G, Grefkes C. Aktivierungswahrscheinlichkeitsschätzung Meta-Analyse der motorischen neuralen Aktivität
nach Schlaganfall. NeuroImage. 2012;59(3):2771-2782.
Rodrigues F. Bento T. Cid L. et al. Kann das zwischenmenschliche Verhalten die Beharrlichkeit und Einhaltung der körperlichen Übungspraxis beeinflussen?
bei Erwachsenen? Eine systematische Überprüfung. Vorderseite Psychol. 2018;9:2141.
Sabaté E. und Weltgesundheitsorganisation. Adhärenz bei Langzeittherapien: Aktionspolitik: Tagungsbericht, 4.-5. Juni 2001.
[online] Apps.who.int. Verfügbar unter: <https://apps.who.int/iris/handle/10665/66984> [Abgerufen am 12. Juni 2021].
Shore C, Hubbard G, Gorely T, Polson R, Hunter A, Galloway S. Unzureichende Berichterstattung über Faktoren im Zusammenhang mit der Überweisung von Übungen
Programmaufnahme, Teilnahme und Einhaltung: Eine systematische Überprüfung von Bewertungen. J Phys Act Gesundheit. 2019;16(8):667-676.
Sieverink F, Kelders SM, van Gemert-Pijnen JE. Klärung des Konzepts der Einhaltung der eHealth-Technologie: Systematische Überprüfung von
Wenn aus Nutzung Adhärenz wird. J Med Internetres. 2017;19(12):402.
Simek E, McPhate L, Haines T. Einhaltung und Wirksamkeit von Heimübungsprogrammen zur Sturzprävention: eine systematische Überprüfung und
Meta-Analyse der Auswirkungen der Eigenschaften von Trainingsprogrammen. Zurück Med. 2012;55(4):262-275.
D. Simpson, M. Bird, C. English, S. Gall, M. Breslin, S. Smith et al. „Die Fernverbindung von Patienten und Therapeuten mithilfe von Technologie ist
machbar und erleichtert die Einhaltung der Übungen nach einem Schlaganfall“. Themen in der Schlaganfallrehabilitation. 2019;27(2):93-102.
Thaker D, Monypenny R, Olver I, Sabesan S. Kosteneinsparungen durch ein telemedizinisches Versorgungsmodell im Norden von Queensland, Australien.
Medizinische Zeitschrift von Australien. 2013;199(6):414-417.
Thompson EL, Broadbent J, Bertino MD, Staiger PK. Beeinflussen schmerzbezogene Überzeugungen die Einhaltung der multidisziplinären Rehabilitation?
: Eine systematische Überprüfung. Clin J Schmerz. 2016;32(2):164-178.
Tierney S., Mamas M., Skelton D. et al. Was können wir von Patienten mit Herzinsuffizienz über die Einhaltung von Übungen lernen? Eine Systematik
Überprüfung qualitativer Arbeiten. Gesundheitspsycholog. 2011;30(4):401-410.
Torriani-Pasin C, Palma GCDS, Makhoul MP, et al. Adhärenzrate, Teilnahmebarrieren, Sicherheit und Gesamterfahrung einer Remote
Programm für körperliche Betätigung während der COVID-19-Pandemie für Personen nach einem Schlaganfall. Vorderseite Psychol. 2021;12:647-883.
Vervloet M, Linn AJ, van Weert JC, de Bakker DH, Bouvy ML, van Dijk L. Die Wirksamkeit von Interventionen mit elektronischen Erinnerungen
zur Verbesserung der Einhaltung chronischer Medikamente: eine systematische Überprüfung der Literatur. J Am Med Inform Assoc. 2012;19(5):696-704.
Vseteckova J., Deepak-Gopinath M., Borgstrom E. et al. Barrieren und Vermittler für die Einhaltung von Gruppenübungen bei institutionalisierten älteren Menschen
Menschen mit Demenz: eine systematische Überprüfung. Eur Rev Alterungs-Phys.-Gesetz. 2018;15:11.
Wendel-Vos GC, Schuit AJ, Feskens EJ, et al. Körperliche Aktivität und Schlaganfall. Eine Metaanalyse von Beobachtungsdaten. Int J Epidemiol.
2004;33(4):787-798.
Yan LL, Gong E, Gu W, et al. Wirksamkeit einer auf der Grundversorgung basierenden integrierten mobilen Gesundheitsintervention für das Schlaganfallmanagement in
ländlichen China (SINEMA): Eine cluster-randomisierte kontrollierte Studie. PLoS Med. 2021;18(4).
Anhang A
PEDro-Schlüsselkriterien für die Qualitätsbewertung:
Festlegung der Zulassungskriterien
Zufällige Zuordnung von Themen zu Gruppen
Versteckte Zuordnung
Gruppen zu Studienbeginn ähnlich bezüglich des wichtigsten prognostischen Indikators
Subjektblendung
Verblindung des Therapeuten
Assessoren blenden
Messung mindestens eines Schlüsselergebnisses von mehr als 85 % der den Gruppen zugeordneten Probanden
Absicht, Analyse zu behandeln
Statistische Vergleichsergebnisse zwischen den Gruppen, die für mindestens ein Schlüsselergebnis berichtet wurden
Punktmaße und Variabilitätsmaße für mindestens ein Schlüsselergebnis
CASP-Schlüsselkriterien für die Qualitätsbewertung:
Wurden die Forschungsziele klar formuliert?
Ist eine qualitative Methodik angemessen?
War das Forschungsdesign angemessen, um das Forschungsziel zu erreichen?
War die Rekrutierungsstrategie den Forschungszielen angemessen?
Wurden die Daten in einer Weise erhoben, die der Forschungsfrage Rechnung trägt?
Wurde die Beziehung zwischen Forschenden und Teilnehmern ausreichend berücksichtigt?
Wurden ethische Aspekte berücksichtigt?
War die Datenanalyse ausreichend streng?
Gibt es eine klare Aussage über die Ergebnisse?
Wie wertvoll war die Recherche?